A little over two weeks ago, M and I flew to Los Angeles from Boston for my parathyroid surgery. The day before surgery, we got to meet the surgeon (hereafter Merlin) that I had been corresponding with and doing tests for since February. Merlin (and his staff) is just as personable in real life as he has been over the phone and via email and it is really nice to finally meet him. We talk in detail about my labs, my symptoms and my other endocrine problems. He discusses with me all of the potential outcomes of the surgery, good and bad – he could go in and find none of my parathyroid glands are bad and we need to continue to search for an explanation for my labs and symptoms, he could find all of my parathyroid glands are bad and need to go, he could find anything in between.
Merlin decides he would like to do an ultrasound of my neck to see whether he can locate any offending parathyroid glands prior to surgery. As is no surprise, having a clear target before you slice someone open is helpful! It takes Merlin all of 30 seconds to locate Little Richard, my big fat rogue parathyroid gland. He showed M and I the images from the ultrasound – my thyroid, this oblong black area attached to the thyroid that is Little Richard – and he explains why he thinks the black area is a parathyroid adenoma. Interestingly, Merlin only sees one area that could be a parathyroid adenoma as he continues the ultrasound on other regions of my neck. The reason this is interesting is that I had an ultrasound in Boston many months earlier, as well as a specialized parathyroid scan called a Sestamibi scan, both to look for parathyroid adenomas.
Sestamibi scans (and ultrasounds for that matter) are notoriously inaccurate methods of locating parathyroid tumors. A well-known parathyroid surgeon, Dr. James Norman, claims: Scans cannot find 50% of parathyroid tumors and when they do, they are wrong 50% of the time. His writing on this topic really is worth a read:
http://www.parathyroid.com/finding-parathyroid.htm
What Dr. Norman describes on his website is remarkably consistent with my experience. I was one of the 50% that had a negative Sestamibi scan. The other interesting point that Dr. Norman makes, is that the results of an ultrasound are only as good as the person conducting the ultrasound! This is kind of a scary truth to hear, but an important one. And it is totally consistent with my experiences as well. I had an ultrasound in Boston at roughly the same time I had the Sestamibi scan at a well regarded teaching hospital. Here is an excerpt from the ultrasound report:
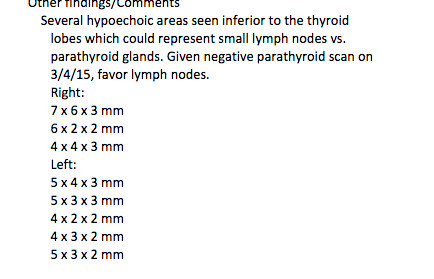 That’s right. There were EIGHT different spots that the doctor conducting the ultrasound thought could either be parathyroid glands (and parathyroid glands are typically only observed on ultrasound if they are hyperplastic or have adenomas because a healthy parathyroid is about the size of a grain of rice and therefore too tiny to see on an ultrasound). And despite the fact that there were EIGHT areas that could be an enlarged parathyroid glands, the ultrasound was read as normal BECAUSE THE SESTAMIBI SCAN WAS NEGATIVE. I thought this was a weird conclusion at the time. If the Sestamibi scan was the only scan that mattered, why bother doing the ultrasound? Wasn’t the point of the ultrasound to catch problems that the Sestamibi scan might have missed? I have never heard of one scan being declared negative because an entirely different scan was negative. That is exactly what this doctor does, however, many months ago. Now do you see why it is so incredibly hard to have this stuff figured out? What happened to me happens to patients all the time – even the good surgeons are aware of it. This is why patients struggle for years to get diagnosed. How are patients supposed to know, without doing a pile of reading, that the results of the scan are purely in the eye of the beholder? Yet again, if I would have believed the radiology reports were the truth, I would have concluded there was nothing wrong with me and I would have stopped trying to chase this down. And that would have been a mistake. ARGH!
That’s right. There were EIGHT different spots that the doctor conducting the ultrasound thought could either be parathyroid glands (and parathyroid glands are typically only observed on ultrasound if they are hyperplastic or have adenomas because a healthy parathyroid is about the size of a grain of rice and therefore too tiny to see on an ultrasound). And despite the fact that there were EIGHT areas that could be an enlarged parathyroid glands, the ultrasound was read as normal BECAUSE THE SESTAMIBI SCAN WAS NEGATIVE. I thought this was a weird conclusion at the time. If the Sestamibi scan was the only scan that mattered, why bother doing the ultrasound? Wasn’t the point of the ultrasound to catch problems that the Sestamibi scan might have missed? I have never heard of one scan being declared negative because an entirely different scan was negative. That is exactly what this doctor does, however, many months ago. Now do you see why it is so incredibly hard to have this stuff figured out? What happened to me happens to patients all the time – even the good surgeons are aware of it. This is why patients struggle for years to get diagnosed. How are patients supposed to know, without doing a pile of reading, that the results of the scan are purely in the eye of the beholder? Yet again, if I would have believed the radiology reports were the truth, I would have concluded there was nothing wrong with me and I would have stopped trying to chase this down. And that would have been a mistake. ARGH!
But I digress. Merlin found ONE abnormality and therefore planned to start the surgery the next day by starting with this abnormality.
Parathyroid surgery is interesting and unusual in the sense that there are typically four parathyroid glands and some may be healthy while others are diseased (hyperplasia or have an adenoma). Some people have more than four glands; some have less. And the parathyroid glands are typically located behind the thyroid but can also appear in other locations as well. Because of this variation in the number and location of the glands, there is also much more uncertainty as to whether finding and removing one bad parathyroid gland will cure a patient with hyperparathyroidism. If a surgeon only looks for and removes one gland, how does he/she know if this is the only problem gland? One way to help resolve this uncertainty is through intra-operative hormone testing. If removing a hyperplastic gland or an adenoma doesn’t cause PTH to drop significantly, the surgeon knows that there is still a problem parathyroid gland somewhere. If PTH does drop significantly (i.e., a drop in PTH of at least 50%), then the surgeon has some reassurance that all of the problem glands have been removed. This is not a completely foolproof system – no system is. But it has been shown to result in a 98 percent cure rate. You don’t have to take my word for this – you can read more about it here:
http://endocrinediseases.org/parathyroid/surgery_pth_monitoring.shtml
To this end, at the beginning of the surgery, Merlin obtained a baseline measurement of my parathyroid hormone (PTH) – the hormone that I had been producing in excess and had been inflating my calcium levels. He then headed straight for the region of my neck on the right side where he found an abnormality on my ultrasound the day before. And lo and behold, he was right – there was Little Richard, my hyperplastic parathyroid gland. He removed Little Richard and retested my PTH. It dropped a little, but nowhere close to 50%. So he kept looking. He could only find one parathyroid gland on my right side, so he went over to the left side of my neck. Both parathyroids were located and looked normal. They were both biopsied to confirm that in fact they were normal and preliminary pathology conducted while I was in the OR indicated that they were normal. These glands were subsequently fitted with little clips so that if they go bad in the future, they are easy to spot, regardless of the skill level of the person that goes looking for them.
At this point, Merlin checked my PTH again and it was still high. So he headed south, into my chest on the right hand side (as this is the side where only one gland had been located so far). Sometimes parathyroid glands can be located deep in the chest, sometimes also in the thymus. I had my thymus removed a few months earlier due to a suspected carcinoid, so that wasn’t an issue for me, but Merlin went down there to take a look anyway. He found a few leftover pieces of thymus that he removed along with 14 lymph nodes. After cleaning out this upper chest cavity, he checked my PTH again. It now dropped by well over 50%. And so, three and one half hours later, Merlin stopped.
I don’t remember talking to Merlin after surgery, as I was still pretty out of it from the anesthesia. But this much was communicated to M, who did get a chance to speak with him. I did get to see all of the details myself about a week after surgery when I was sent a copy of the operative report. The operative report was quite interesting. Here is the summary:

Wait. What? THYMIC MASS? I had my thymus removed in June and no tumor was identified in pathology. Granted, I got better, so I didn’t believe that. But a piece of thymus was left in my chest and that leftover piece had a mass? I read further into the report because I can’t quite believe this and see it very clearly says Merlin saw a “nodular mass in the superior tip of my thymus” which was still sitting there in my chest.
I want to be clear – the reason I am showing you pieces of my reports is because this whole thing seems so outlandish to me that I wouldn’t believe it if someone just told me this story. I would want proof. So, I am showing you the reports so you can see I am not just making this shit up or exaggerating or adding my own twist to the story for dramatic effect. This is really, truly happening. I barely believe it myself most days – and I am living it.
Of course, the pathology on this thymic mass came back as normal thymus tissue. But given what happened after thoracic surgery in June, I am of course suspicious of the pathology. But who knows? Perhaps this is all incidental? I may never know the answer to that question. I am just going to be glad that Merlin found it and took it out, along with my bad parathyroid gland, and I will leave it at that for now.
